Time to read 40 minutes
In July 2021's EarTalk Webinar, Value Hearing founder and audiologist, Christo Fourie, explains hearing loss. This 30 minute webinar covers types, causes, prevalence, symptoms, impact, diagnosis and treatment of hearing loss.
Watch the video or read the transcript below.
So welcome, everyone, this, I believe, is our sixth EarTalk webinar, and today I'd like to talk about hearing loss in a bit more detail, discussing the types, the causes, prevalence, etc.
And I just want to thank Dr. Raza Hashimi from our Perth clinic, who created these slides for me while they were in lockdown. So that's been very helpful.
When it comes to hearing loss, we will look at the definition of hearing loss. We will look at the different types of hearing loss. We'll look at the various causes and we'll look at the impact hearing loss has financially and personally on people. We’ll look at the prevalence of hearing loss, how it's diagnosed, and also treatment, which isn't always just hearing aids, and then we’ll go into the most common types and as well as the symptoms they present with some types could be considered medical emergencies, others not.
And it will cover the most common types as well as the more serious types of hearing loss causes as well.
Understanding hearing loss
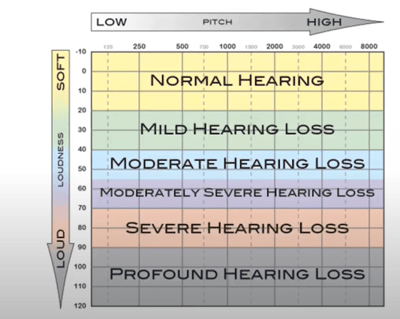 So as you may have seen with my previous webinar, where we spoke about hearing loss and I used a tool to explain hearing loss. We test hearing on an audiogram, which is a graph plotting the softest sound you can hear down the Y axis, and the pitch on the X axis. So on the left hand side of the graph, you've got low pitch. On the right hand side, you've got high pitch.
So as you may have seen with my previous webinar, where we spoke about hearing loss and I used a tool to explain hearing loss. We test hearing on an audiogram, which is a graph plotting the softest sound you can hear down the Y axis, and the pitch on the X axis. So on the left hand side of the graph, you've got low pitch. On the right hand side, you've got high pitch.
And the further down the marks made on the graph, the worse the hearing. And then we can classify the hearing loss from normal hearing through to profound hearing loss. And that's a standard set internationally.
Sensorineural hearing loss
Sensorineural hearing loss is probably the most common type we deal with. It's a permanent hearing loss where the nerves or the hair cells in the inner ear are damaged. It's irreversible.
Although they are looking at stem cell therapies to try and improve that kind of hearing loss, they haven't had a good breakthrough yet. There's always some sort of issue in resolving them. And it feels like most studies say in ‘10 years time’. They've been saying that for the last 20 years. So eventually there will be something, but not quite yet.
Conductive hearing loss
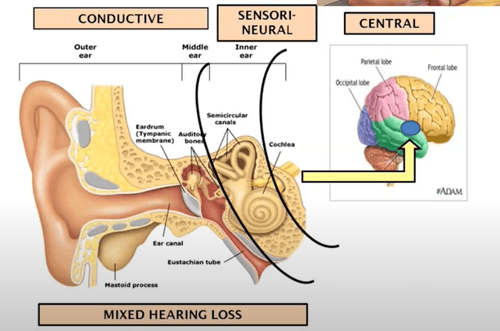 Conductive hearing loss is essentially more in line with visual loss. So, the reason people wear glasses (is to use a lens to correct vision. In this type of hearing loss) the ‘lens’ of the ear, or the middle ear, is impaired and essentially stops transmission from sound from the outside through to the inner ear where it can be processed.
Conductive hearing loss is essentially more in line with visual loss. So, the reason people wear glasses (is to use a lens to correct vision. In this type of hearing loss) the ‘lens’ of the ear, or the middle ear, is impaired and essentially stops transmission from sound from the outside through to the inner ear where it can be processed.
Typically, we call that conductive hearing loss and it's typically treated surgically or medically. In some cases where surgery risk is too great for the benefit, hearing aids can work wonderfully for this kind of hearing loss.
Mixed Hearing Loss
Mixed hearing loss is where someone might have a nerve related hearing loss as well as a middle ear issue overlaying on top of it.
And that could then mean a combination of treatments - the medical part, taking care of the conduct of components, or the blockage part, and then hearing aids, taking care of any remaining sensorineural or nerve related loss attached to it. Or in some cases where they can't do surgery, hearing aids have to address the whole loss itself.
Central Hearing Loss
Central hearing loss is a relatively newer type of hearing loss.
It's not that it has not existed, but our definition of it has changed. The problem isn't in the ear itself - although it could also be - (but) it's the way the brain processes the signal coming into the ear. And typically that kind of hearing loss presents with a very poor speech understanding no matter what you do with hearing aids.
It's quite a difficult and challenging hearing loss to deal with because nothing you do on the ear is going to fix the brain's ability to interpret what's being said and increase the understanding.
Even cochlear implants can't help much there. Luckily, not that common, but it's something to be aware of because you could have a normal hearing on the periphery but have central hearing loss, but most commonly you've got sensorineural hearing loss and, due to the lack of stimulation over years, you also then have a disconnect of the nerves in the brain, which leads to poorer speech understanding.
And that poor understanding isn't always recoverable when you put hearing aids in or implant someone with a cochlear implant, for instance.
Hearing Loss Causes
Sensorineural
So there are many causes of sensorineural permanent hearing loss.
As you can see, it's anything from ageing, being hit on the head - where you’ve got a skull base fracture, for instance - noise exposure, virus infections, mumps, measles. Even some people with flu get what is called idiopathic sensorineural hearing loss, which is a sudden hearing loss - shingles, medications that damage the ear, typically chemotherapies or certain types of antibiotics. Meningitis, which is an infection of the brain or the brain membranes and diabetes because it affects the blood flow to the ear, similarly, stroke. Meniere’s disease, which is a disease on the ear, acoustic neuroma, which is a cancer on the hearing nerve itself and then genetics and several other factors.
So there's no one factor for any kind of hearing loss specifically. And some factors could present quite similarly on the audiogram.
Conductive
Conductive causes- the blockage hearing loss. There are many causes and many reasons for it - outer ear infection or middle ear infection, which is simply glue ear. Kids typically suffer with that quite constantly, particularly because in children, the structure of the eustachian tube, which is supposed to dry the middle ear, is still tiny and it's more flatly oriented so it doesn't drain as well. So kids tend to get more middle ear infection than adults.
Swimming could cause outer ear infection, using dirty ear plugs, picking at your ears all sorts of things can cause pain and swelling of the canal, which can block off the canal. Scarring or perforation of the eardrum, using cotton balls and punching a hole through the eardrum or a hit to the head or ear, which puts a blast of air pressure that tears that little eardrum.
Even excess wax build up can block your ears. Otosclerosis, which is a genetic condition where this abnormal bone growth on their little bones, which gets them fixated.
Putting things in your ear. I'm sure you've read many stories where someone discusses or finds a 20 year old bus ticket rolled up in someone's ear.
Poor eustachian tube function is essentially, again, the tube that drains the middle ear in some adults, you've got what we call eustachian tube dysfunction which never drain properly and that can cause all sorts of fluctuations and blockages in the ears, which sometimes is better and sometimes worse.
Sinus can cause issues blocking that little tube and then you can have genetic malformations of the ear, which can affect the structure as well. So many, many causes of blockage or conductive type hearing loss.
Mixed Hearing Loss
And that also comes into mixed hearing losses.
You can have both the conductive cause and sensorineural causes, which gives you a mixed hearing loss. Symptoms of hearing loss is quite common. Hearing loss from different causes might have the same symptoms.
This relates more to the acoustic symptoms. So people sound like they’re speaking muffled. You could also have distortion of speech, which is typically a more serious issue. So if that happens, do see your doctor.
If you suffer hearing loss, you've probably had all of those. And it definitely relates to the shape of the audiogram or your hearing test result. It relates to which sounds you hear well and which you don't hear as well, and how those symptoms might present. And not everyone will experience the same symptoms and not everyone will experience the symptoms to the same extent either. So it's important to understand that as well.
Hearing Loss Impact
So the impact of hearing loss has been studied several times, and there’s definitely a financial impact. There's a study they brought out in Australia that showed someone with hearing loss or untreated hearing loss loses about $11,000 a year in income due to missed opportunities due to the hearing loss itself. So it has a financial impact, but it also has social and emotional impact in that you cannot necessarily do as well in social groups.
You might withdraw from those groups. You might suffer depression because of that withdrawal. So it has a snowballing effect.
So it's quite an important issue for many people, although some people just write it off as’ I'm getting older, people just need to stop mumbling or don't stick their head in the cupboard when they speak to me’. But there's a lot more going on.
We're also now seeing more and more evidence linking untreated hearing loss to an increased risk for cognitive decline, things like Alzheimer's disease. And there's some studies that show even a mild hearing loss increases your chance of Alzheimer's disease by one point nine times, which is quite significant for even a very mild hearing loss. For more severe hearing loss, it gets up to close to five times more likely to develop Alzheimer's because of the lack of stimulation on the brain.
So it is more than just an invisible problem. It has real impact on people's lives.
Hearing Loss Prevalence
The prevalence is quite great in general, we can say around 10% of the whole world's population has hearing loss. It's definitely more prevalent in adults than in children. And there's millions of people who suffer from hearing loss, but only about 20% of people who actually could benefit from hearing aids use them. And that's due to various reasons. It could be financial, although when we looked at finances in Australia, for instance, the prevalence of hearing aid use is low in the pensioner group as well, even though in Australia we've got Hearing Services Program which essentially can give free hearing aids to eligible pensioners. And despite being able to get them for free, there's still people who choose not to get them.
That's not due to price alone. There's other factors playing a role, and that's really the nut people need to crack to get on top of this hearing loss issue.
Hearing Loss Diagnosis
So when it comes to hearing loss diagnosis, it typically involves going to their doctor first, but a proper diagnosis would be a hearing test with an audiologist or an audiometrist, which starts by taking your history. And all that means is we ask you some questions to understand your work history, noise exposure, health history to understand where hearing loss might impact you.
That gives us a good overview of what to expect of the testing. Then we can reference the testing to what you gave us in the interview, or the test history, and see how everything fits together. And that can help with a differential diagnosis. But a hearing test doesn't just consist of a beep test. We need to look at things like looking in the ear, obviously, to see if there's any blockages or other issues involved.
We need to sometimes look at tympanometry, which is a pressure test - where we can see if we pick up signs of conductive or blockage loss - and see where the problem lies so we can write a medical report and get you referred on if appropriate.
Then we get to the beep test, where we look at your ability to hear beeps at different levels and find the softest sounds you can just hear. But we might also do a bone conduction test and typically, for a comprehensive test, we would test your hearing through the skull; that part bypasses the outer and middle ear and stimulates the nerve directly. And we can then compare results through the skull versus through the ear and see if there's a difference which would show up a conductive component or blockage component in your hearing..
We use speech audiometry to assess how well your brain understands speech once we've corrected for your loss. And that could indicate issues of central hearing loss, which is where the brain doesn't understand what's being said.
And we do also do speech-in-noise assessment to really understand how the brain deals with competing noise in difficult situations, which becomes important once you make recommendations around hearing aids, so you can find a hearing aid that's most likely to work for you in those challenging situations.
Hearing Loss Treatment
So treatment of hearing loss very much depends on the type of hearing loss.
If it's an infection, typically your doctor would recommend a treatment - a cream or antibiotics - for it. If the eardrums burst, they might do surgery to repair the eardrum. If you've got fixated little bones, there is surgery available that can cut the bone and replace it with a little piston that takes over the function so it's not blocked anymore.
Grommets are little tubes you can put in the ear to stop the issue of eustachian tube dysfunction, where the tube ventilating the middle is not working. They put a little tube through the eardrum and it equalizes pressure through that tube, rather, through the eustachian tube, and that works very well. They might remove tumours through surgery. And then a lot of hearing loss is actually treated with hearing aids.
And, if the hearing loss gets to a point where hearing aids aren't working anymore, there's also options of cochlear implants.
For some hearing loss, we might have discharge in the ears. So hearing aids get blocked all the time. They might do bone conduction hearing aids where they just implant a little prosthesis, which clips onto a vibrator which literally vibrates the skull like the bone conductor and the sound travels through the skull rather than through the ear.
And then certain hearing loss, like sudden onset hearing loss - where you suddenly lose your hearing, you get tinnitus, everything sounds distorted - that needs very quick treatment, typically within 24 hours by a doctor and might involve steroids if prescribed. And then obviously hearing aids.
There's other assistive listening devices you can use things like remote microphones, FM systems to really address the needs you have in a variety of situations because hearing aids, as discussed in previous videos, have a limited range. So if you need to hear in specific situations, there's usually things you can add to the hearing aid to help you for that specific situation as well.
Common Types of Hearing Loss
What I'd like to do next is just go into the most common types of hearing loss, which we tend to see. And also I'm going to go to some important ones which we don't see often, but are very important for you to understand what to do when you experience these sorts of symptoms.
Noise Induced Hearing Loss
So with noise induced hearing loss, it's probably one of the most common ones we see. In the past, before there was regulation requiring hearing protection, we found a lot of men - more prevalent in males than females - due to work, had noise induced hearing loss.
And what that means is part of a hearing might be perfectly normal, but the high frequency part has this notch in it. Essentially, loud noise comes in. It travels along the cochlea, which is a little spiral, and all that energy is lost on that first curve of the spiral, which relates to the hair cells in the inner ear, which serve the high frequencies.
So the common symptoms for noise induced hearing loss is, ‘I can hear fine as long as it's not a female voice or a child's voice, as long as you're not looking away from me, as long as there's no background noise’ because it's not a loss volume, as such, it's a loss of clarity.
You can hear what people are saying, but you can't distinguish what's being said. If you're looking at someone, there might be enough information to get the information off the lips, even though you're not trained in lip reading. The brain uses whatever it can get. But if you're not looking at someone, then the loss of high frequencies is really going to affect you.
Fortunately now with legislation, we are really moving away from work-induced noise related hearing loss. But what we are seeing take up that space is self-induced/noise induced hearing loss where people use headphones and turn them up way too loud and you're causing hearing loss that way.
And also loud concerts where if you're standing in front of a speaker and be there only for about ten minutes before it causes damage. So a lot of young people are exposing themselves to that kind of noise. Even people with noise induced hearing loss working on farms for themselves without hearing protection, are having that kind of hearing loss.
So it is very important you protect your hearing in noise because it can, and most likely will, cause noise induced hearing loss.
There is some very small percentage of people who don't suffer it as badly. It seems to be a genetic link, but it's a small fraction of people who could tolerate that noise and not have much damage. But you don't know, so best to protect your hearing.
You can't get your hearing back.
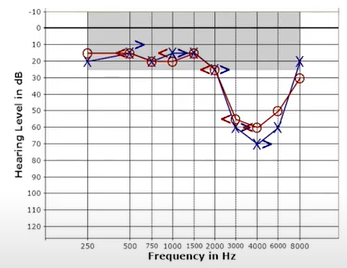 That's the graph you see there is a pure noise induced hearing loss, but again, it could be combined with an age hearing loss which could be combined with the conductive hearing loss. So this is just a pure noise induced hearing loss.
That's the graph you see there is a pure noise induced hearing loss, but again, it could be combined with an age hearing loss which could be combined with the conductive hearing loss. So this is just a pure noise induced hearing loss.
Typically, tinnitus might be part of it because you can hear the high pitched sounds, just a nerve firing most likely to be a high pitched, in that kind of hearing loss.
Hearing aids these days work very well for that kind of hearing loss, which wasn't traditionally the case. It was very hard to address only the high pitch without causing issues in the low pitch or causing whistling in the hearing aids. But modern hearing aids over the last 10 plus years have been very, very effective at treating this kind of hearing loss.
So important to know, because a lot of men from that generation will still suffer with that kind of hearing loss from work.
Age related hearing loss
Age related hearing loss is another very common one. One thing to understand is just because you're getting older and there is hearing loss associated with it - and certainly the older you are, the more likely you are to have hearing loss - but doesn't mean that it's normal.
You still have impaired hearing, but it might just be more prevalent in your age group.
Typically, it's to do with wear and tear, not specifically to noise per se. And there's a variety of causes.
It would generally appear to be a more gradually sloping loss or a flat loss. But again, you have an age-related overlay on top of a noise related hearing loss, which could change this graph altogether.
And as you can see, the prevalence is quite large over 65 and that increases as you get older. So at 90, it's going to be about 90 percent prevalence of hearing loss. So there is definitely an age related component there as well.
Normally, hearing aids work very well for this kind of hearing loss. And the symptoms might relate to where your loss is great. And in this case, this person's volume for the low pitch might be reduced, but they've got a lot of problems with the clarity as well. And we certainly would have to look at the person's speech understanding to see how well they might do with hearing aids both quiet and in noise.
Sudden onset hearing loss
This one is really what I wanted to bring into today's webinar. It's something that's not often understood by GPs even, but essentially what it is, it's a very sudden hearing loss where you wake up one morning and the hearing in one ear appears to be gone.
If you do hear anything, it's quite distorted. You might have an echo or certain sounds like a zing or squeak or all sorts of weird sounds. It's not always associated with pain in that ear, but your ear might feel blocked because you're not getting any sound in.
If you experience any of those symptoms, and it's happened very suddenly, it's very important to see your GP and talk to them about sudden hearing loss.
What I've unfortunately seen is some GPs might then prescribe antibiotics, even though the ear appears clear and they usually give it a week and then check again and then they send you to a specialist.
But this kind of hearing loss typically needs steroid treatment within hours - within the first 24 hours - to have any chance of success.
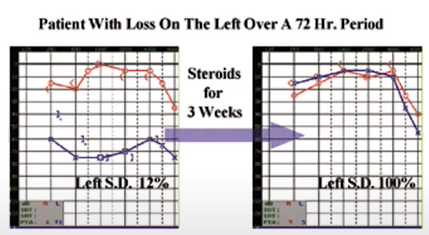 Steroids, as you can see on this graph, can recover a lot of the hearing or most of it in many cases. But without steroid treatment for this kind of hearing loss, and quick steroid treatment for this kind of hearing loss, It's unlikely you're going to get much recovery.
Steroids, as you can see on this graph, can recover a lot of the hearing or most of it in many cases. But without steroid treatment for this kind of hearing loss, and quick steroid treatment for this kind of hearing loss, It's unlikely you're going to get much recovery.
So, if you experience any symptoms of a fullness in the ear, sudden change in your hearing overnight, that doesn't get better when you try and equalize your ear, for instance, without any pain in the ear, not necessarily ringing distortion in one ear, then that is a reason to see a doctor or even go to a hospital's emergency department because they seem to be more likely to get you onto the nose and throat specialist to recommend steroids.
It's not something you can go to a chemist for either. Audiologists can’t recommend steroids.
It has to be your doctor, but certainly an audiologist can do the test and do the referral. But whether or not you're going to get into an audiologist within those 24 hours, that's a good question as well.
So, very important to be aware if anything changes very quickly in your hearing, particularly if there is distortion. Get in to see your doctor and don't just accept antibiotics as the answer because if it's this kind of hearing loss, it might leave you with permanent damage to that ear.
And typically the speech understanding with this kind of hearing loss is terrible. So hearing aids don't work particularly well for this kind of hearing loss
Acoustic neuroma
Another not particularly common type of hearing loss is something called acoustic neuroma, or Schwannoma - in this case, the Vestibular Schwannoma - would create a balance disturbance. The auditory nerve, the hearing nerve that runs between the brain is only 2cm long and it runs through a little bony canal. Typically, it's a cancerous growth, but it's a benign cancer. So it's not going to kill you. It essentially just takes up space. So that nerve runs through a little channel in the bone.
And if there's a growth on that nerve, that growth pushes out against the bone, but obviously can't push into the bone. So it starts pushing into the nerve. And as it pinches that nerve, it can create hearing loss and it could also create balance disturbance. So typically, you could have a slow (hearing loss) development of one ear, dropping gradually over time. And that's why it's important to see an audiologist if you've got hearing loss, because they can monitor your hearing over time.
It might be linked to a single sided tinnitus or ringing in one ear, and it typically becomes worse and worse and worse over time. It may or may not include vestibular system issues which relates to balance disturbances, dizziness, nausea, that sort of feeling. But that's not always the case. Sometimes it just presents as a hearing loss. Sometimes it might just present as a balance disturbance. So, again, it's important to see an audiologist if you have any hearing loss, particularly if it's one ear alone, as it tends to trigger a few red flags.
So if you've got a hearing loss in one ear, or significantly worse in one ear, I can only encourage you to see an audiologist because we need to perform that differential diagnosis to try and figure out whether it is something serious you need to be referred on, to see a doctor or an ENT to get some clarity on that loss.
You don't know until you know.
Meniere’s Disease
Meniere’s disease, something we see fairly commonly. It tends to be a genetic disease, but also some studies have described it or assigned it to people who are a bit more stressed, essentially. It's also single-sided hearing loss and it typically involves fluctuation in hearing.
So some days you might hear better, other days your hearing might drop and it would also normally be associated with some sort of distortion. It's not just like things get softer, but it might also have squeaky noises or echoes going on in the ear.
It's very commonly also associated with low pitch tinnitus.
People describe it as a rumbling, an ocean-like noise, and it's to do with excessive pressure build-up in the inner ear which tears the little membrane in the inner ear itself, in the cochlea.
The fluids mix, the electrical potential changes, your hearing drops until that membrane heals again and the hearing might go back up again. But over time the hearing loss gets greater and greater and greater, up to a point where the Meniere’s might stabilize.
The Meniere’s might be only Cochlear, in which only the hearing loss that fluctuates. It might be classic Meniere’s, which both has a hearing loss but also has a very disturbing symptom of nausea, room spinning, associated with a Meniere’s attack. Or it might be vestibular Meniere’s where your hearing isn't affected, but you do suffer the vestibular system balance disturbances - the nausea, the room spinning, which is quite awful.
Typically, people with this kind of loss, especially if it includes vestibular symptoms, tend to end up going to the GP or referred to an ear, nose and throat surgeon and these medications that can help you manage your Meniere’s disease with a good bit of advice for this kind of fear loss, which is quite common, is just to avoid salt because salt can build up more pressure on the ear, although I wouldn't stick to just that.
Definitely see a doctor if you do have any symptoms like that.
And again, it brings to light the fact that if one ear is different to the other ear, that's a trigger to go see a specialist, an audiologist, a GP.
If it's a sudden change in hearing, go to your doctor. If it's a slow change see an audiologist, we can then refer you to your doctor after doing the diagnosis because the doctor's going to need those results in any case.
Otosclerosis
So otosclerosis is another kind of hearing loss that tends to affect one ear first and it might then involve the other ear later. So essentially it's a genetic condition that tends to be more prevalent in females than males. It often happens after or during pregnancy because there's more calcium flowing through the body to help the baby. And what happens is the last little bone in the ear, the stapes, sits on a little membrane. As sound hits the ear from it, vibrates through and vibrates the little membrane. But around that membrane is bone, so that the bone of the little stapes gets connected to the bone of the skull.
Basically you might have calcium deposits through that little ring that separates the two and that starts fixating. This last little bone is fused so the vibration of the eardrum doesn't go through to the fluid of the inner ear properly. And as those fixations increase, that bone gets more and more stuck, which means your hearing loss will increase over time.
What will happen then is your hearing loss will get worse and worse and worse. Gradually over time, it might involve tinnitus. It doesn't typically involve pain but it might involve a fullness in the ear because your ear feels blocked and it might only be in one ear. We often see it on the left ear instead of the right ear for some reason we don't quite understand.
As it gets worse, that calcification might actually go into the inner ear and start involving a nerve related loss as well. The kind of surgery that works well for, is called the stapedectomy, where they essentially cut the little stapes off then drill little hole through the remaining footplate of the stapes and then put a little piston that rests on that membrane and tie that piston onto the two other bones that carries vibrations through. The risk of that is quite large.
You need to speak to specialists about it. They might actually recommend hearing aids prior to going down the surgery path because hearing aids work extremely well for this kind of loss, because all it is, you just need more power to cross that fixation. And you hear really well even with more basic hearing aids.
Again, a single-sided hearing loss that needs investigation.
Middle Ear Infection
Middle ear infection is a very common one for children. Also, some adults might have suffered hearing loss due to infections over the years and years and years. So they know who they are. They are typically under care of a specialist by that time because it could be quite painful as the pressure builds up.
It's important that it's treated though, because the middle ear is very close to the brain. And obviously anything that's infecting the ear could eat through the skull and cause meningitis as well over time.
That's not something you just leave.
Children will often report with a middle ear infection and it's easily fixed. Normally a doctor would try antibiotics and if that doesn't work, or if it is a consistent issue, they might use grommets, which is the tube that drains the fluid and the pressure through the ear canal rather than through the eustachian tube which is dysfunctional in this kind of hearing loss.
So quite a common one, and particularly in children, but also found in some adults. So hopefully that covers the main types of hearing loss for you.
